Clinical Controversy
In a study by Lin et al., there appeared to be no difference in success rates when comparing patients who underwent sympathetic nerve clipping compared to cutting. Coelho et al., produced similar results, showing no differences in success rates, compensatory hyperhidrosis.
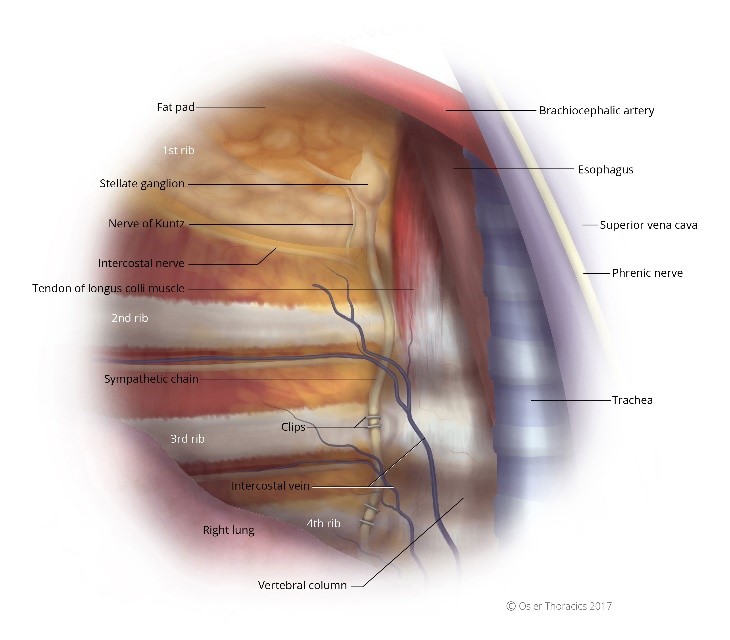
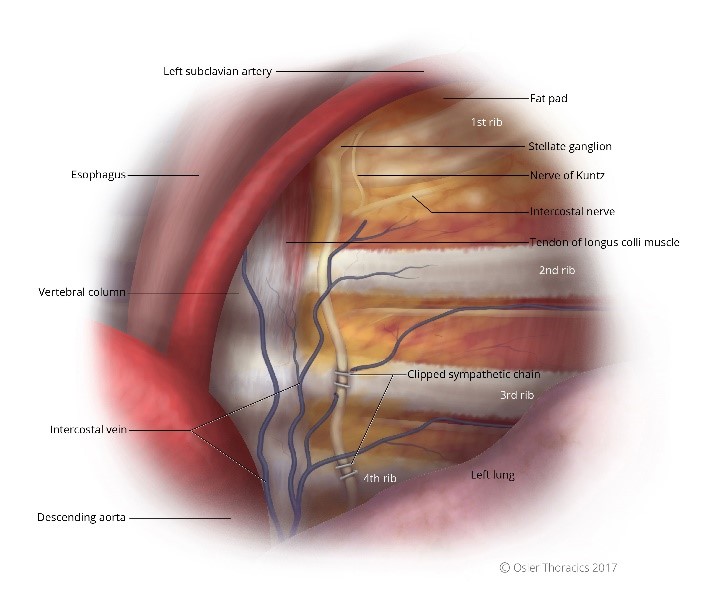
Figure 6: (a) Right intrathoracic view, the sympathetic chain clipped; (b) Left intrathoracic view, the sympathetic chain clipped.
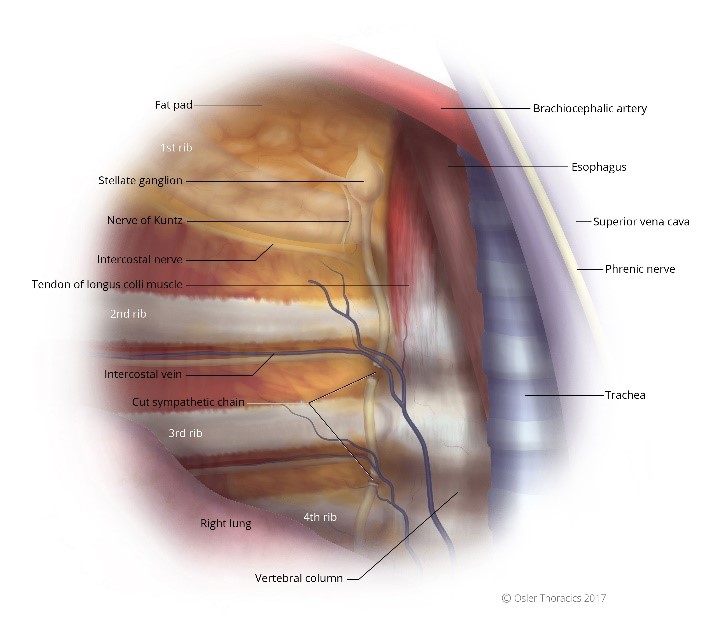
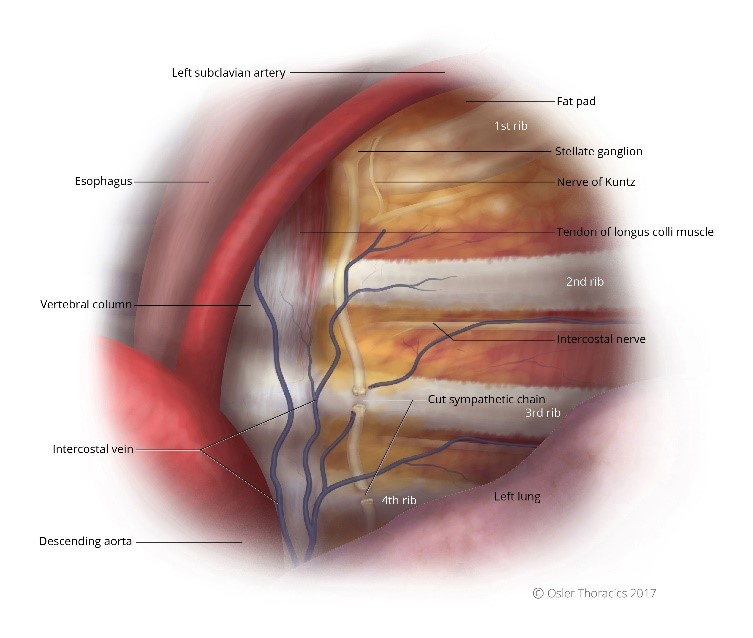
Figure 7: (a) Right intrathoracic view, the sympathetic chain cut; (b) Left intrathoracic view, the sympathetic chain cut.
In 2014, Panhofer et al. compared clipping at cutting at R4/R5, finding that clipping was less effective but interestingly resulted in decreased rates of compensatory hyperhidrosis.
At TSC, we feel that clipping provides a false sense of security, inappropriately promising reversibility if compensatory hyperhidrosis is too severe. This may soften stringent physician screening for ETS, resulting in an increase rate of poor outcomes. At TSC, we tell patients that clipping the sympathetic nerve should be considered permanent with no clear evidence of reversibility. We believe that the only true window of reversibility is within four weeks of the procedure. As we are very careful in choosing our surgical patients, we recommend sympathectomy over clipping as we feel the clinical results are superior.
Clinical Pitfall
It is critical to discuss all non-surgical options prior to consenting the patient for surgery. These include:
| Non Surgical Option | Details | Targeted Area | PROS | CONS |
|---|---|---|---|---|
| Botulintoxin A | Botox from Allergan | Axillae Palmar | Minimal Risk Very Effective | sts 5-6 months Can cause temporary hand weakness Costly |
| Iontopheresis | Electrical current on the skin | Palmar Plantar | Minimal Risk Can reduce symptoms by 70-80% | Requires treatment every 48 hours until therapeutic Requires maintenance Costly device |
| Microwave Thermolysis | miraDry® | Axillae | Minimal Risk Can reduce symptoms by 80-90% Reduces hair growth Permanent | Costly Often requires 2 treatments Temporary local irritation of skin |
| Glycopyrrolate | Avert | Total Body | Effective in treating total body hyperhidrosis | Dry mucous membrane Many systemic side effects Many drug interaction |
Clinical Tip
We all recognize the risk of compensatory hyperhidrosis after VATS sympathectomy. However, less common side effects should be also discussed to ensure your patient is properly educated prior to proceeding with surgery.
Reduction in Resting Heart Rate
Papa et al. studied the effect of sympathectomy on resting heart rate and systolic blood pressure. At 30 days and 2-year follow-up, both variables were reduced, similar to the effects of beta-blockers. Others have demonstrated a similar response, however, with no impairment of exercise capacity or cardiorespiratory response to exercise.
This response is likely secondary to the division of small nerve fibers that provide autonomic sympathetic innervation to the cardiovascular system.
Horner’s Syndrome
As the level of sympathetic nerve disruption is no longer T2, the risk of Horner’s syndrome has dropped dramatically. After performing well over 1200 ETS procedures we have not had a single occurrence of Horner’s syndrome. Patients who suffer from this complication complain of drooping of the upper eyelids, constriction of the pupils, and dryness of the eyes. Although exceedingly rare, it should be discussed with your patients.
Gustatory Hypherhidrosis
Gustatory sweating is another side effect which occurs in about 5% of cases. This condition, in which patients notice that they tend to experience increased sweating while eating or smelling certain foods, develops in rare instances.
Typically, patients will complain of sweating over their lip when they eat spicy foods.
Temporary Return of Symptoms and Phantom Sweating
A short time after the operation, 3 to 4 days, approximately 5 % of patients will complain of a temporary recurrence of their palmar hyperhidrosis. Although this is a short-lived phenomenon that may last 1-3 days, they must be informed about this possibility as it may lead to panic and doubt.
Many patients also complain of “Phantom Hypherhidrosis”. They describe a sensation of impending palmar hyperhidrosis, however the sweat never develops. This phenomenon tends to dissipate over a few months.
Clinical Pitfall
Redness in the face can be more disabling than hyperhidrosis. When flushing is easily triggered, patients tend to avoid social interaction leading to social phobias, depression and anxiety.
We have found those that present with facial flushing are frequently tearful during consultation and are desperate for a “cure”. It is therefore very critical to exhaust all non-surgical options prior to ETS. Surgery for flushing has more severe compensatory hyperhidrosis when compared to those with hyperhidrosis. Patient satisfaction with the outcome of surgery also decreases with time.
Exhaust Non-Surgical Treatment
Pharmacological Intervention
Consider SSRIs to reduce flushing and social anxiety. Beta blockers have also been use with success. Topical NSAIDs to treat the flushing can also be considered.
Cognitive-Behavioral Therapy
Many patients have already attempted this prior to a consultation with a thoracic surgeon.
Communicate the risk of severe compensatory hyperhidrosis and Horner’s syndrome:
As the sympathetic nerve is clamped at T2, the risk of injury to the stellate ganglion is real. Also, the higher you interrupt the chain, the higher the severity and frequency of compensatory hypherhidrosis. We have also noticed that the risk of gustatory hypherhdrosis is higher in this cohort of patients.
In a study by Smidfelt et al., 73.5% were satisfied, 11% were dissatisfied, and 15.5% regretted the operation.
Conclusion
Although ETS is a simple technical procedure, the decision to operate represents the most difficult challenge for thoracic surgeons.
Patients drive this part of a surgeon’s practice, frequently requesting the referral from their family doctor. They present to the office emotionally charged, and ready to commit to surgery. However, the onus is on the surgeon to carefully weigh the pros and cons of ETS, especially since the side-effect of a poorly selected patient can be devastating.
In properly chosen patients, ETS can change the course of their lives. They can become more engaged socially and professionally. Surprisingly, they are frequently more grateful to you than many of your oncology patients.
Full references available upon request.